I still recall the first time Richard Lilford proposed using theatre within healthcare service design. My response was not immediate excitement, but a blend of curiosity and caution. Forum Theatre? In a sector that thrives on protocols, guidelines, and measurable outcomes, the idea felt unusual, even risky.
My professional life has been rooted in research and clinical education, where every new approach must endure the test of peer review. In this environment, good ideas are not enough; they must be supported by evidence, evaluated with precision, and implemented with clear purpose. Yet, the thought of using theatre to explicate the complexities of healthcare stayed with me.
Theatre holds a particular strength as it draws people in and creates a space where emotions, perspectives, and lived experiences meet. I began to ask myself: could this approach go beyond artistic expression? Could it genuinely help shape services that function better and enable patients to make informed choices?
When I began piloting Forum Theatre in maternity care, I quickly understood that introducing something so unconventional in a high-stakes environment is not an easy undertaking. It is creative, yes. It is engaging, certainly. But the question of whether it can truly transform practice remains more complex and perhaps the answer will only emerge over time.
Why Theatre? The Promise
Healthcare decision-making is rarely straightforward. Patients navigate not just medical facts, but personal beliefs, time pressures, and the emotional weight of uncertainty. Traditional communication tools, such as leaflets, consultations, and even decision aids, can be useful, but they often struggle to convey the lived experience behind a choice.
This is where theatre offers something different. Through enactments, role reversals, and freeze-frame interventions, it allows participants to pause, reflect, and re-frame conversations. In service design, it can highlight bottlenecks in the patient journey that might otherwise be invisible. In patient decision aids, it can bring abstract concepts to life illustrating not just what a decision is, but how it feels.
There are precedents, too. Applied theatre has been used effectively in medical education to teach empathy and communication skills.[1] In some healthcare projects, small-scale interventions have engaged marginalised communities in mental health discussions or helped staff reflect on unconscious bias.[2] The literature here is modest but intriguing, suggesting that theatrical methods can open doors to dialogue that conventional tools sometimes fail to unlock.
In my own pilot work, I’ve seen moments that are hard to ignore. A clinician, watching an enactment of a rushed antenatal consultation, suddenly recognised how her own phrasing might be perceived as directive rather than supportive. A service user spoke openly about how the performance helped her feel “heard” in a way that traditional focus groups never had. These moments remind me why the idea is worth exploring.
The Reality Check – The Challenges
But here’s where my reflective side kicks in: moments are not outcomes. And in healthcare, outcomes matter.
Firstly, not every audience engages in the same way. Some clinicians embrace the opportunity to experiment; others find it contrived or even uncomfortable. Patients may respond differently depending on cultural norms, previous experiences, or simply their mood that day.
Secondly, measuring impact is complex. Theatre excels at sparking insight, but translating that into tangible, measurable change in service design or patient decision-making is another challenge entirely. Did a performance actually lead to better-informed patients? Did it alter the structure of a service? Without robust evaluation, it’s easy to overestimate its effect.[3]
Thirdly, context matters. In some settings, the time, resources, and willingness to try something so unconventional may simply not be there. Even with support, integrating theatre into service design requires careful facilitation, clear objectives, and a realistic plan for follow-up.
I’ve had moments where I questioned whether the outcomes justified the energy spent on organising an enactment. Once, after a performance that I felt was powerful, a participant simply shrugged and said, “It was interesting, but I’m not sure what I’ll do differently.” That’s a humbling reminder that innovation alone doesn’t guarantee transformation.
The Middle Ground – Balanced Reflection
So where does that leave us? Somewhere in the middle and that’s not a bad place to be.
Theatre is not a magic wand for healthcare service design. But it’s also not a gimmick. It is a tool, and in my view, one that can be powerful in the right circumstances, with the right preparation, and the right follow-through.
In our pilot work, the value wasn’t in replacing existing methods, but in complementing them. Theatre didn’t replace patient surveys, structured interviews, or decision aid prototypes. Instead, it enriched them. It provided texture, nuance, and a safe environment for participants to express things they might never articulate in a survey form.
One example stands out. We staged a consultation about induction of labour for a large-for-gestational-age baby. The scene played out as scripted, but then we invited the audience to “freeze” the moment and suggest alternative approaches. This simple pause shifted the dynamic entirely. Clinicians experimented with different tones of voice. Patients challenged medical jargon. The dialogue became more collaborative not because we’d given them new facts, but because we’d created space to try new ways of interacting.
Did this lead to measurable change in patient decision-making? I can’t claim it did, at least not yet. But it certainly influenced how participants thought about their roles in those conversations. Sometimes, that’s the necessary first step.
Looking Forward – What Experts Should Consider
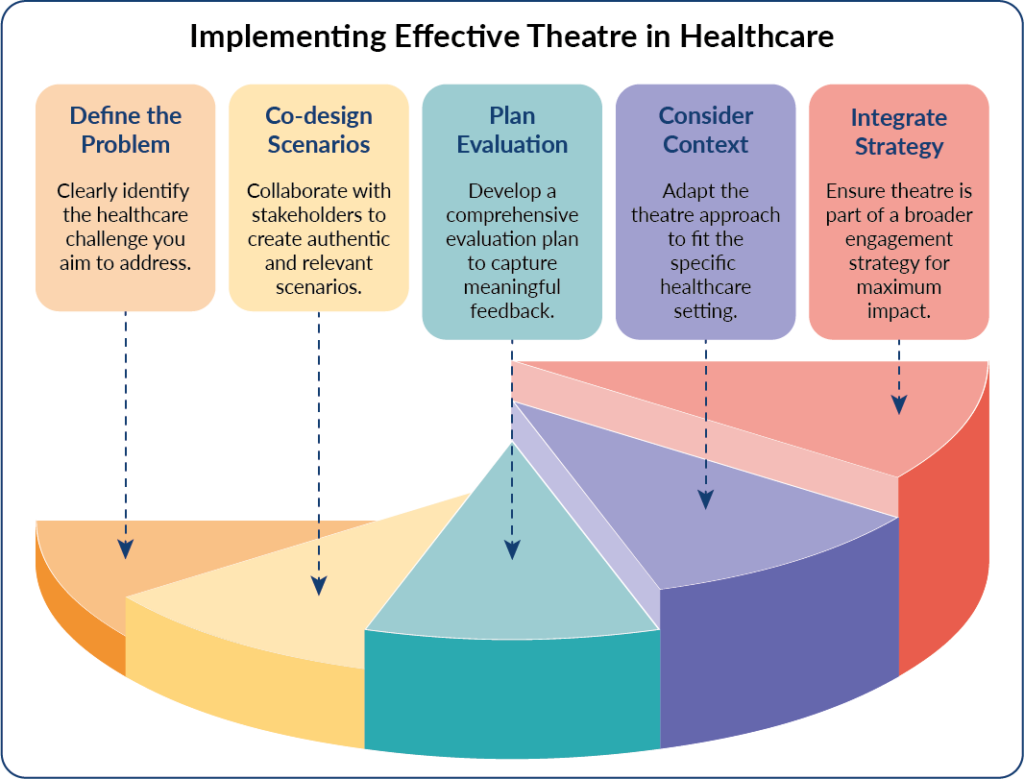
For those in the field considering theatre as part of service design or designing patient decision aids, we’d suggest a few principles:
Start with the ‘why’: Be clear about the problem you’re trying to solve. Theatre is a means, not an end.
Co-design from the start: Work with patients, clinicians, and facilitators to shape scenarios that are authentic and relevant.
Plan for evaluation:Whether qualitative, quantitative, or mixed methods, ensure you can capture more than just “good feedback.”
Think about context:Not every setting will embrace theatre – adapt to the culture, constraints, and readiness of the environment.
Integrate, don’t isolate:Theatre works best as part of a broader engagement strategy, not as a standalone event.
If we approach it with humility and curiosity, theatre could become another tool in our collective toolkit for improving healthcare design and patient support. It may not always be the right tool for the task, but still one worth having.
Closing: The Final Note
When I first stepped into this space, I thought I might find a clear answer: yes, theatre works or no, it doesn’t. The truth, as is often the case in healthcare, is more nuanced.
Theatre has the potential to change perspectives, spark empathy, and create moments of clarity. But it’s not a guarantee. It may not “do the job” in every context, and that’s okay. What matters is that we stay open to testing new approaches while holding ourselves accountable to providing evidence and impact. In fact, when we think about why patient decision aids often fall short, three recurring barriers keep emerging: time constraints, limited health literacy, and the constant threat of information overload all of which our theatre approach is designed to tackle head-on.[4]
For me, the real value has been in the conversations that followed the moments when someone said, “I hadn’t thought about it that way before.” Those are not outcomes you can easily plot on a graph, but they are the seeds of change.
And perhaps that’s the point. In a field where we are constantly seeking certainty, theatre reminds us that some of the most important shifts begin with uncertainty and the courage to try.
— Saba Tariq, Post-doctoral Fellow; Pamela Nayyar, Research Project Manager
References:
- Landry-Wegener BA, Kaniecki T, Gips J, Lebo R, Levine RB. Drama training as a tool to teach medical trainees communication skills: A scoping review. Acad Med. 2023; 98(7): 851-60.
- Beckett K, Deave T, McBride T, et al. Using Forum Theatre to mobilise knowledge and improve NHS care: the Enhancing Post-injury Psychological Intervention and Care (EPPIC) study. Evidence & Policy. 2022; 18(2): 236-64.
- Lilford RJ, Nayyar P, Tariq S. Supporting patient choice: Design decision aids or design a service. NIHR ARC West Midlands and Midlands PSRC News Blog. 2025; 7(3): 1-3.
- Tariq S. The three musketeers of patient decision aids: Time constraints, health literacy, and information overload. NIHR ARC West Midlands and Midlands PSRC News Blog. 2025; 7(3): 5-7.