The Problem
Most work concerning methods to support patient choice concerns decision aids.[1, 2] A decision aid is a tool to help people make informed choices among healthcare options. It provides evidence-based information about the potential risks and benefits of different interventions and helps clarify what matters most to patients. Within the NIHR Midlands PSRC, and with support from NIHR ARC West Midlands, we are reviewing the literature on decision aids to inform choice in pregnancy. We have found 18 studies comparing decision aids with care as usual. These studies cover various choice scenarios, such as planned caesarean section vs planned vaginal delivery after a previous caesarean, and choice of birth for a large baby.
All studies showed benefits for the decision aids compared to care not supported by the decision aids, over various scaled outcomes, such as knowledge, satisfaction with care, and satisfaction with the decision made. Whilst the studies described the interventions in detail, accessing the decision aids proved challenging due to a lack of relevant permissions required for access and inactive links to websites where the information was originally available. While a few studies (e.g. Kuppermann, et al. [3]) included the decision aid in the Supplementary Material, we can find no evidence that the decision aids that were the topic of enquiry in the various studies have been sustained in practice.
Furthermore, a decision aid does not function in isolation from the service – staff have a role in providing psychological support and in answering questions, no matter how good the decision aid artefact may be. Clinical staff have a duty to inform people of their options, and then they are responsible for carrying through the selected management plan. Yet there is more literature on decision aids as an artefact than on staff education to support patient choice, irrespective of whether a decision aid was or was not deployed. A rare exception is an education package to improve decision support in the field of cardiovascular medicine. [4, 5]
All of the above considerations lead to a conclusion that what is needed is service design to support patient choice by providing a complete package of structures and processes to support choice, and to integrate decision aids into a coherent package. So, what are the elements that should be included and how should they be integrated? To make our task tractable, we will situate our endeavour in the context of common option sets that arise in the third trimester of pregnancy.
A Service to Support Patient Choice in the Third Trimester of Pregnancy
The components of an integrated choice support service are represented in the Figure.
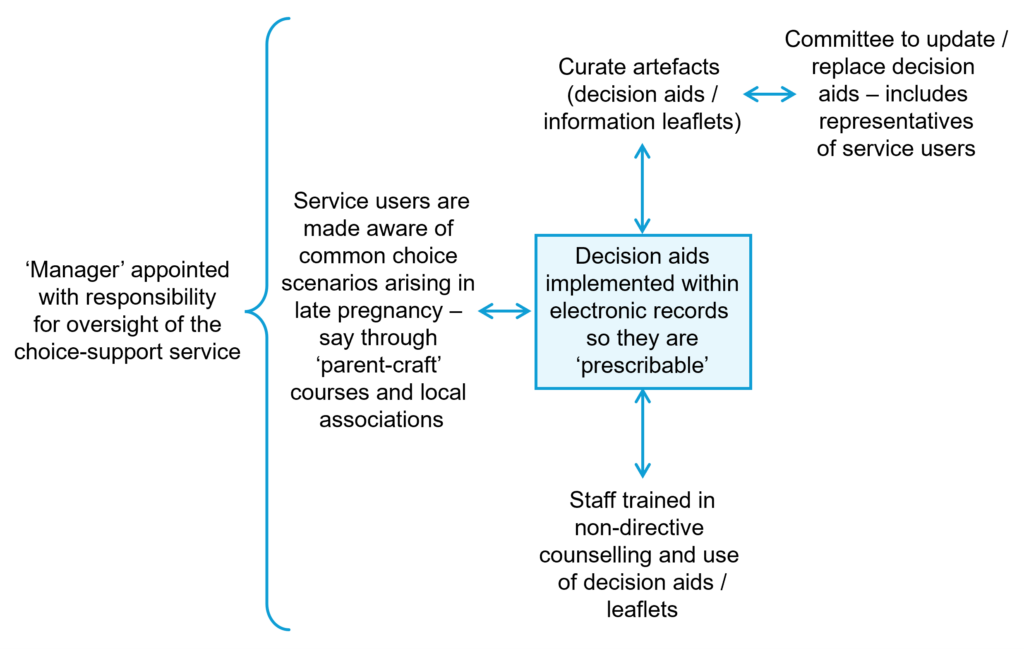
Figure: Representation of a Choice Support Service
These components consist of the following:
1. Decision Aids
Given that decision aids are effective, their use should be supported by the service. Services should therefore select a set of evidence-based and institutionally-endorsed decision aids. The set should include aids dealing with common decision scenarios, such as mode of delivery (e.g. for persistent breech presentation, putatively large baby, previous caesarean section) and place of delivery (e.g. home vs midwife unit vs obstetric unit). Ideally, the decision aids should conform to the International Patient Decision Aid Standards (IPDAS), which cover issues such as the optimal method of presenting probabilistic information.
2. Selection of Decision Aids
Many of the above choices are catered for by existing decision aids. However, knowledge evolves, and decision aids may therefore become obsolete. The corollary is that the service needs to implement some type of standing committee or management structure to ensure that a selection is made from those available (ideally from professional societies or official bodies such as NICE in England). The service should be free to make justified amendments to these aids and to participate in national or international endeavours to produce or update decision aids.
3. Curation of Decision Aids
The above cannot be a one-off exercise but must be repeated and updated at regular intervals. The selection and maintenance of the decision aid library should be a service function, analogous to the maintenance of the pharmaceutical inventory. Thus, a member of staff should assume overall responsibility for the service and should be assisted by an advisory committee.
4. Ensuring Availability of Decision Aids
As stated above, decision aids, like clinical guidelines, are ephemeral in the sense that they tend to disappear and become inaccessible. This problem can be easily solved now that the services are replete with electronic notes. Thus, decision aids should be incorporated in the notes so that they are ‘prescribable’ when the need arises. Again, the management structure suggested above could be responsible for selection, maintenance and incorporation of decision aids.
5. Staff Education
Offering patient choice is not a simple or straightforward matter since it is time-constrained, must balance information volume with overload, and cater for different levels of health literacy (see the following article).[6] Thus, staff training should be encouraged as a crucial part of Continuing Professional Development. Such training may benefit from role-play and/or video-presentations of choice scenarios under different constraints. Such role-play can introduce strategies for coping with challenges, such as time constraints or a situation where the decision-makers feel overwhelmed. For example, the strategy of offering a further appointment where the decision-maker is invited to bring a relative or friend, or when an interpreter may be present.
6. Advance Notice
While simulating choice scenarios in our work programme, it became apparent that there are several choice scenarios to which a sizable proportion of the pregnant population will be exposed. For example, some services set the definition of a predicted large baby at the 90th centile, meaning that approaching 10% of the population, for whom an intervention is not otherwise indicated, will be offered a choice of birth method. Some may argue that the choice of an alternative birth method should be offered (not just open) to all women. These considerations invite the question ‘why wait until the scan has shown a large baby before introducing the choice?’ Therefore, we would invite readers to consider the idea that all pregnant women should have some advance warning of choices that often arise closer to the time of birth, and of some of the benefits and risks of alternatives – sources of further information could be made available at this time. At least we think that the option of ‘advance notice’ should be discussed with service users. Such a service may be particularly useful for people with special needs.
7. Managerial Oversight and Governance
One member of staff – such as a specialist obstetrician or consultant midwife – should be designated to assume overall responsibility for the patient information service. This person should report to the board through the institution’s overall governance structure.
Conclusion
In this article we advance the argument that offering choice is a subtle art that needs to be built into the overall design of maternity services. Our proposed service design is represented in the above figure. Safety has a nuanced meaning in the context of choice – safety is not simply a question of minimising risk. It is a question of selecting the option that minimises the overall risk arising from each individual risk weighted by its preference.[7] Offering choice in a non-directive emotionally supportive way is one of the most difficult parts of practice. It is a task that should be supported in the way services are designed.
— Richard Lilford, ARC WM Director & Midlands PSRC Co-Director;
— Pamela Nayyar, Research Project Manager;
— Saba Tariq, Post-doctoral Fellow.
References:
- Lilford RJ. Decision Aids to Help People Make Difficult Decisions. NIHR ARC West Midlands and Midlands PSRC News Blog. 2024; 6(5): 1-4.
- Lilford RJ. Implementing Decision Aids in Routine Clinical Pathways. NIHR ARC West Midlands and Midlands PSRC News Blog. 2025; 7(1): 1-3.
- Kuppermann M, Kaimal AJ, Blat C, et al. Effect of a Patient-Centered Decision Support Tool on Rates of Trial of Labor After Previous Cesarean Delivery: The PROCEED Randomized Clinical Trial. JAMA. 2020; 323(21): 2151–9.
- Pollak KI, Olsen MK, Yang H, et al. Effect of a Coaching Intervention to Improve Cardiologist Communication. A Randomized Clinical Trial. JAMA Intern Med. 2023; 183(6): 544-53.
- Lilford RJ. One-to-One Coaching Improves Cardiologists’ Communication Style. NIHR ARC West Midlands News Blog. 2023; 5(4):6.
- Lilford RJ. The Information Paradox at the Heart of Non-Directive Counselling. NIHR ARC West Midlands and Midlands PSRC News Blog. 2024; 6(4): 1-3.
- Lilford R, Girling A, Stevens A, Almasri A, Mohammed MA, Braunholtz D. Adjusting for treatment refusal in rationing decisions. BMJ. 2006; 332(7540): 542-4.